|
|
|
|
|
|
|
|
Biointegration
|
|
|
|
|
|
|
Components of the implant
An implant normally consists of two parts:
1) The part of the implant that will be inserted into the bone during surgery is called the fixture. The fixture is shaped like a hollow screw. The bone will grow onto surface of the fixture.
2) The part of the implant that breaks through the mucosa (the gum) is called the abutment. The abutment is anchored in the fixture by means of a screw. Above the gum the abutment carries the tooth replacement. The abutment can be shaped in many ways, depending on which function and tooth replacement are needed.
|
|
 |
|
 |
|
|
Biotechnology
Implants are made of the metal titanium in an almost pure form. Titanium's ability to be integrated in the bone has been known for more than 25 years. Years of experience and research form the basis of the knowledge and use of implant technology today.
|
|
|
|
|
|
 |
 |
|
|
|
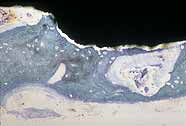
Oseointegration of an implant is a direct structural and functionally stable connection between the living bone and the surface of an implant that is exposed to mechanical load.
Biointegrationen in the bone usually lasts 3-4 months in the lower jaw and 5-7 months in the upper jaw. If the implant is placed in an area where a bone augmentation has been performed, it may be necessary to postpone the loading of the implant.
|
|
|
The survival rate of an implant under optimal conditions is at least 96% after 5 years (i.e. 96 out of 100 implants are in function for at least 5 years). The few implants which do not integrate are normally lost during the first year. After the first year, the risk of losing an implant is very small when the implants are properly cleaned (good oral hygiene).
Many implant clinics will offer the patients some kind of guarantee for the implant treatment.
|
|
|
A successful implant treatment depends on:
|
|
|
1. The height and width of the jawbone in the area receiving an implant. The bone must have a certain size to achieve a good result.
|
|
|
2. The bone quality may vary due to medicinal or hormonal conditions, but is also different in the same person depending on the anatomical location. These conditions are evaluated when the treatment is being planned by the dental surgeon.
|
|
|
 3. The shape and structure of the implant affect the implant's ability to integrate into the bone and keep the bone level around the implant when it is functionally loaded. 3. The shape and structure of the implant affect the implant's ability to integrate into the bone and keep the bone level around the implant when it is functionally loaded.
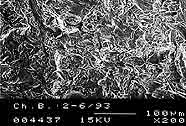
The greater the diameter of the implant , the greater the contact area that is obtained to the surrounding bone.
Different techniques are used to produce a rough surface on the different types of implants. The area of the rough surface on the picture is increased 3 times compared to the smooth untreated titanium surface.
|
|
|
4. Immediate loading of the implant after the placement into the jawbone is normally avoided for at least 3 months. Microscopic movements of the implant in the bone can cause delay or destroy the ability of bone to create a stable connection to the titanium surface. However, a limited loading of the implant after the placement is acceptable, but only in cases where a primary stability of the implant is obtained after the placement procedure.
When the implant is integrated in the jawbone, the amount of functional loading is a critical factor for the survival of the implant. For example, a treatment with a large bridge construction on an insufficient number of too short implants may result in a loosening of the implants or the abutments.
|
|
|
5. Infection in the wound in relation to the implant placement is very rare and is not considered critical for the survival of the implant.
Infection of the gum and the bone after the implants have been functioning in the mouth (periimplantitis) can on the other hand be the reason for the loss of implants. Periimplantitis is normally the result of inferior oral hygiene of the implants that support the crowns, bridges or dentures. This is the reason why it is very important to keep the implant supported constructions thoroughly clean.
|
|
|
|
|
 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
